
This web page was created programmatically, to learn the article in its authentic location you possibly can go to the hyperlink bellow:
https://www.nature.com/articles/s41371-025-01051-3
and if you wish to take away this text from our web site please contact us
Search outcomes
Following de-duplication, the database search resulted in 5302 titles and abstracts (Fig. 1). After overview based mostly on titles and abstracts, 426 full textual content articles have been assessed for eligibility, leaving 17 research included within the ultimate evaluation. 12 of those had adequate knowledge for meta-analysis.
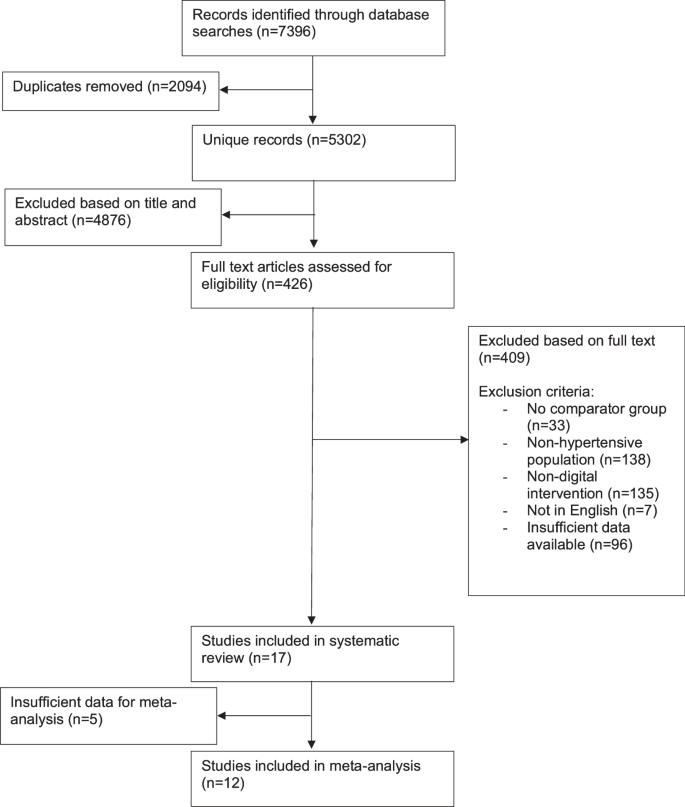
Flowchart of included research.
Study traits
Characteristics of the 17 included research are outlined in Table 1. The research have been performed in a variety of nations. Most research have been performed in outpatient [18,19,20,21,22,23,24,25] or neighborhood [26,27,28,29,30,31] clinics.
The pooled pattern measurement for change in systolic blood strain was 3040 contributors (vary 30 [32] to 493 contributors [24]). Most research included contributors based mostly on a earlier prognosis of hypertension [18, 20,21,22,23, 25, 26, 28,29,30, 33, 34], with some specifying this to be >140/90 mmHg [22, 33] or ≥140/90 mmHg [18, 22, 23, 25, 30, 33]. The relaxation included people based mostly on screening go to blood strain readings ≥135/85 mmHg [31], ≥140/90 mmHg [24, 27, 32], or >140/90 mmHg at a earlier clinic go to [19].
Intervention length ranged from 3 months to 12 months. Only two research adopted contributors up past the tip of the intervention. Both had interventions lasting 3 months however adopted up their contributors at 6 months [30] or 12 months [18]. The outcomes on the finish of the intervention interval have been included within the meta-analysis, as both there was an choice so as to add treatment after the tip of the intervention interval [30], or later end-point values weren’t given for every group [18].
The nature of the digital intervention diverse amongst research (Table 2). Six research used multi-faceted interventions that concerned contact with a healthcare skilled in addition to a digital intervention (e.g. web site entry and nurse phone counselling) [19, 21, 22, 26, 29, 34]. The remaining 11 research had totally automated digital interventions, with no direct involvement from a healthcare skilled [18, 20, 23,24,25, 27, 28, 30,31,32,33]. Eight research had interventions that concerned contributors self-monitoring their blood strain [19, 22, 24, 27, 30,31,32, 34].
Control interventions diverse between research. Three research had typical care as a comparator [23, 26, 28]. Ten research had gave hypertension life-style recommendation in a ‘non-digital’ format, with eight offering written recommendation [18, 20, 21, 24, 27, 30,31,32] and two research offering in-person hypertension training to manage teams [19, 29]. Four research gave management contributors entry to a restricted component of the digital intervention acquired by the intervention group [22, 25, 33, 34].
11 research had change in blood strain as their major final result [19, 22,23,24,25,26,27, 30,31,32,33]. The remaining six had blood strain measurement as secondary outcomes, with major outcomes being change in BMI [18], change in weight [21], proportion of sufferers assembly pre-specified targets (glycated haemoglobin <7%, systolic blood strain <140 mmHg, or low-density lipoprotein ldl cholesterol <130 mg/dL) [20], research feasibility [28], and adjustments in well being behaviour [29, 34].
Methods of blood strain knowledge assortment included averages of repeat blood strain measurements taken throughout research visits [18, 22, 24,25,26, 28, 31, 33, 34], self-reported residence readings [19, 32], measurements taken in the neighborhood [27], 24-hour ambulatory blood strain measurements [30], and was unspecified in 4 research[20, 21, 23, 29].
Risk of bias
Results from the danger of bias evaluation are summarised in Fig. 2. Six research had a excessive threat of bias in a minimum of one area [19, 20, 23, 26, 27, 34], and threat of bias was unclear in a minimum of one area for the rest. Where excessive threat of bias was current, this was mostly resulting from attrition bias. Of these research included within the meta-analysis, three had a excessive threat of bias [23, 26, 27].
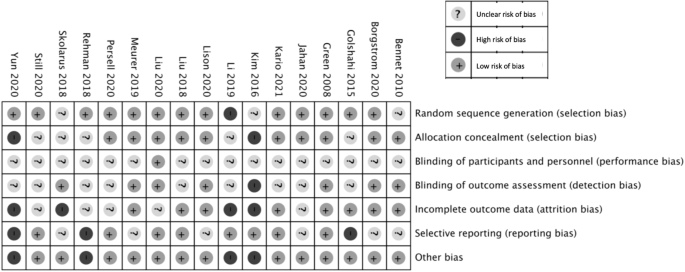
Risk of bias abstract: overview authors’ judgements about particular person threat of bias domains for every included research.
Primary final result
Systolic blood strain
Eight research carried out statistical evaluation evaluating the change in systolic blood strain between intervention and management teams [22, 24,25,26,27, 30, 31, 33], of which 4 discovered a major discount with the intervention [24, 26, 30, 33]. Three research in contrast distinction in systolic blood strain change between a number of teams [23, 28, 29], with two discovering a major distinction between teams [23, 29]. One research reported a major distinction within the proportion managed <140/90 mmHg between teams [20]. The remaining research didn’t evaluate blood strain outcomes between teams.
Ten research reported a imply change in systolic blood strain from baseline to finish level for each intervention and management teams [18, 23,24,25,26,27, 30,31,32,33] (See Supplementary Digital Content 2). Two additional research reported baseline and finish level blood strain values for each teams, from which a imply change and normal deviation was calculated [22, 34]. These 12 research have been included within the meta-analysis (Fig. 3). The remaining 5 reported inadequate numerical knowledge for inclusion [19,20,21, 28, 29]. Blood strain readings from research visits have been reported and utilized by 10 of the research [18, 22,23,24,25,26,27, 31, 33, 34]. The remaining two research reported participant self-measured blood strain, and these values have been included within the meta-analysis [30, 32].
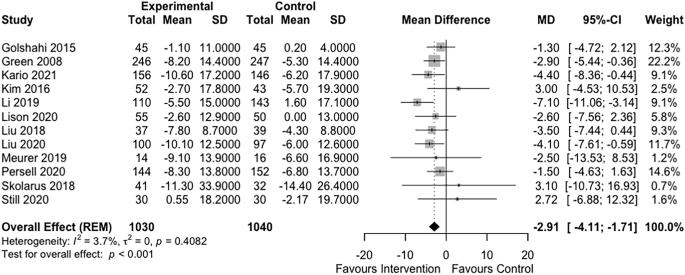
Forest plot of the impact of digital interventions focusing on life-style components for hypertension on systolic blood strain.
The forest plot in Fig. 3 summarises the impact of intervention on systolic blood strain. Digital interventions have been related to a statistically vital discount in systolic blood strain in comparison with management (imply distinction (MD) −2.91 mmHg; 95% confidence interval (CI) −4.11, −1.71; p worth (p) <0.001; I2 = 4%, τ2 = 0).
Subgroup evaluation
Larger research (pattern measurement >100) had a higher impact measurement than smaller research: imply SBP distinction −3.22 mmHg (CI−4.45, −1.98) vs 1.86 mmHg (CI −3.02, 6.4) respectively, p < 0.05 (Fig. 4). No vital variations between subgroups have been seen based mostly on use of residence blood strain monitoring (p = 0.97), intervention length (p = 0.91), nature of management group (p = 0.41) or clinician involvement (p = 0.7) (see Figures, Supplementary Digital Content 3–6).
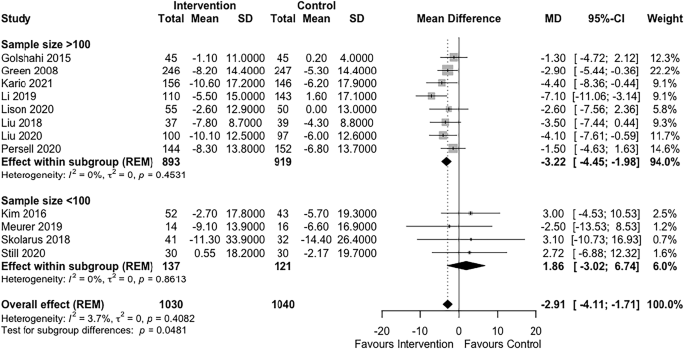
Subgroup evaluation of impact of pattern measurement on systolic blood strain final result.
Sensitivity evaluation
A post-hoc sensitivity evaluation was undertaken. A major distinction in change in systolic blood strain was seen even when research with unclear threat of bias in additional than 2 domains, or excessive threat of bias in any area have been faraway from evaluation (−3.20 mmHg; CI −5.13, −1.26; p = 0.001) (see Figure, Supplementary Digital Content 7). A funnel plot of research included within the meta-analysis didn’t counsel reporting bias in favour of the intervention. Most smaller research didn’t present a blood strain lowering impact (see Figure, Supplemental Digital Content 8).
Secondary outcomes
Ten research included adequate knowledge for inclusion in a meta-analysis of diastolic blood strain [18, 22,23,24,25,26,27, 30, 31, 34]. The imply distinction in diastolic blood strain change between teams was −1.13 mmHg (CI −1.91, −0.35), p = 0.005, I2 0%, τ2 = < 0.0001 (see Figure, Supplementary Digital Content 9).
Reporting of different secondary outcomes was too heterogeneous between research to permit meta-analysis (see Supplementary Digital Content 10). Three research reported the change in BMI between teams [28, 30, 31], one in all which discovered a statistically vital enchancment in BMI with the intervention (−0.2 kg/m2, CI −.4 to −0.1, p = 0.005) [30]. Of three research that reported values for weight change [21, 22, 30], just one carried out an evaluation to check teams, and located a major distinction (−0.5 kg, p = 0.003) [30]. Four research carried out statistical evaluation evaluating bodily exercise measures between teams [20, 25, 31, 33], with one discovering a major distinction in bodily exercise (p = 0.02 for distinction in day by day steps at 12 months) [33]. Reporting for salt consumption (5 research [23, 29, 30, 33]), and/or dietary outcomes (5 research [23, 25, 29, 31, 33]) used completely heterogenous outcomes. One research discovered a major discount in salt consumption within the intervention group in comparison with management (p < 0.001), utilizing verify sheets crammed by contributors to measure salt consumption. All research reporting dietary outcomes discovered both no vital distinction [25, 31, 33] or didn’t carry out statistical evaluation [23, 29]. Outcomes regarding smoking have been solely reported by two research, every with a distinct measure [23, 34]. Neither in contrast between group adjustments in smoking measures.
This web page was created programmatically, to learn the article in its authentic location you possibly can go to the hyperlink bellow:
https://www.nature.com/articles/s41371-025-01051-3
and if you wish to take away this text from our web site please contact us

