1. Introduction
The confluence of declining start charges and elevated life expectancy has led to inhabitants ageing being positioned as one of many central points dealing with well being programs at the moment [
1,
2]. While start charges are declining, enhancements in healthcare programs and social assist, political and financial stability, and the promotion and adoption of wholesome existence have led to elevated longevity among the many international inhabitants [
3,
4]. However, this improve in longevity has additionally been linked to poorer well being through the last years of life, rising the chance of creating continual illnesses comparable to heart problems, most cancers, or neurodegenerative issues [
5]. Consequently, there’s at the moment a excessive comorbidity of continual illnesses amongst older adults, which ends up in a decline in high quality of life and hinders unbiased functioning [
6,
7]. Moreover, the incidence of continual well being situations constitutes the first explanation for mortality, notably among the many older inhabitants [
4,
5,
6,
7].
In this sense, ageing might be interpreted as a tough achievement given the prolongation of life expectancy and, on the similar time, as a problem to be overcome by well being care and financial programs [
4]. For this purpose, essentially the most broadly accepted definitions of wholesome ageing give attention to preserving the talents that allow people to operate independently of their setting and obtain well-being [
8]. In explicit, sustaining cognitive functioning allows people to work together with the setting correctly and protect their high quality of life [
9,
10].
Cognitive modifications throughout previous age might symbolize each a normative ageing course of and a scientific or pathological efficiency [
11,
12]. The first one is characterised by a decline in advanced duties that require consideration, visuospatial, velocity info processing and a few elements of reminiscence and govt features [
13,
14]. On the opposite, cognitive modifications in older maturity might also point out a pathological trajectory, progressing from Mild Cognitive Impairment (MCI) to dementia. MCI is widely known as an intermediate stage previous dementia, characterised by cognitive signs that start to noticeably intervene with on a regular basis functioning [
15,
16,
17]. Dementia, in flip, includes extra pronounced cognitive deterioration, is related to poorer psychological well being outcomes, and represents one of many main causes of incapacity worldwide [
18,
19]. According to present literature, each cognitive decline and dementia have been proven to have a considerable influence on a person’s means to carry out actions of every day dwelling. These actions, which can embody instrumental duties comparable to utilizing the phone, getting ready meals, or scheduling medical appointments, in addition to primary self-care actions like bathing or dressing, are all considerably compromised by these situations [
20,
21,
22,
23].
For its half, different well being situations that would come up all of the sudden, comparable to Parkinson’s illness and stroke, might outcome within the impairment of a number of or some cognitive domains. Regarding Parkinson’s illness, it constitutes the second most typical neurodegenerative dysfunction, and complete circumstances worldwide are anticipated to extend from 11.9 million in 2021 to 25.2 (95% CI 21.7–30.1) million in 2050 [
24,
25]. Although Parkinson’s illness is characterised by impaired motor expertise, analysis signifies that sufferers with Parkinson’s have considerably poorer cognitive efficiency than the overall inhabitants, and that poorer cognitive efficiency is related to worse scores on postural instability and gait problem [
26]. Cognitive impairment on this section of the inhabitants happens extra in all probability and critically in superior phases of the illness, in older people and seems abruptly [
27,
28]. Lower efficiency of duties involving govt features, language and reminiscence is often discovered amongst these people, together with a subjective feeling of slowed pondering [
29,
30,
31,
32].
Regarding stroke, it consists of a cerebrovascular occasion characterised by the blood movement obstruction to a area of the mind [
33]. In this case, prevalence charges vary from round 3% amongst younger adults and an estimated 7.7% amongst people older than 65 years previous [
34]. After a stroke, it’s actually laborious to foretell the diploma of impairment and the cognitive domains affected, as it will rely on the situation of the lesion, the dimensions of the instantly affected tissue and the extent of harm past the ischemic core. A significant a part of cognitive signs after a stroke occasion is expounded to govt operate and language-communication skills, in circumstances the place frontal or temporal areas are affected [
35]. However, visuospatial and perceptual-motor features are concerned when the parietal space is affected [
36,
37]. In addition to cognitive signs, temper can also be affected by the looks of hysteria and depressive signs after the stroke [
38].
The heterogeneity noticed throughout diagnostic situations displays the broader actuality that cognitive decline is formed by a fancy interaction of organic vulnerability, well being standing, and lifestyle-related elements. Several threat elements have been related to worse cognitive trajectories, together with environmental exposures [
39], cardio-metabolic situations comparable to heart problems, diabetes, and weight problems [
40], and modifiable behaviors comparable to bodily inactivity or substance misuse [
41]. Conversely, engagement in intellectually stimulating and socially significant actions has been recognized as protecting in opposition to cognitive deterioration [
42,
43]. Educational attainment additionally performs a vital position, contributing to cognitive reserve and mitigating the scientific expression of pathological cognitive decline [
44,
45,
46]. Importantly, these elements don’t have an effect on all people equally. Different well being situations work together with life-style and sociodemographic traits to provide distinct patterns of cognitive impairment [
47]. For instance, vascular threat elements might disproportionately affect govt functioning in stroke survivors, whereas mental engagement might exert stronger protecting results in neurodegenerative situations [
48]. To perceive these protecting or threat results, you will need to be aware that, whereas mind upkeep refers back to the preservation of bodily integrity, cognitive reserve implies the upkeep of functioning. In this sense, the cognitive enrichment framework offers a mechanistic bridge between life-style and these constructs [
49].
Considering variability in cognitive trajectories and the distinct patterns related to totally different diagnostic teams, standardized remedy approaches could also be inadequate. Increasingly, scientific tips advocate for person-centered care fashions that tailor interventions to the person’s cognitive profile, well being standing, life-style, and private objectives [
49]. This sort of orientation requires deep data of particular person traits and the context through which sufferers are located [
50,
51]. As person-centered remedy is outlined within the literature, it should not solely be based mostly on data of particular person traits, however a joint decision-making course of should even be established amongst sufferers, formal caregivers, and their households [
52,
53]. In this sense, individualized remedy in circumstances of pathological cognitive decline permits for an enchancment in particular expertise as a way to obtain essentially the most unbiased every day functioning potential, as said in earlier research [
54]. Likewise, one of these remedy has been proven to scale back signs of agitation in individuals with dementia, which significantly improves their high quality of life [
55]. In this regard, from the attitude of cognitive enrichment, it’s postulated that the presence of people in stimulating environments not solely correlates with higher efficiency but additionally facilitates processes associated to neural plasticity, comparable to elevated synaptic density [
56,
57].
In this examine, we geared toward inspecting the potential moderator results of diagnostic teams on the explanatory results of life-style and sociodemographic indicators on particular cognitive domains. By doing so, this analysis strikes past inspecting primary results to check whether or not diagnostic standing moderates these well-established associations. After establishing the mannequin for the overall pattern utilizing information from the newest launch of the SHARE undertaking, we are going to additional discover the measurement invariance throughout normative, dementia, Parkinson and stroke teams. Lifestyle results are anticipated to vary between teams as a result of larger sensitivity of scientific teams in entrance of normative situations. Additionally, the supervening nature of stroke situation leads us to consider that this inhabitants could also be extra predisposed to restoration than degenerative teams, comparable to these identified with dementia and Parkinson’s illness.
3. Results
3.1. Descriptive Statistics
The information confirmed distinct profiles throughout the 4 examine teams concerning demographics and life-style habits. The normative group was the youngest on common (M = 64.83, SD = 8.62) and had the very best instructional attainment (M = 12.18 years, SD = 3.96). Women represented 55.1% of this group. This group additionally confirmed essentially the most lively life-style profile: almost three-quarters engaged in bodily exercise greater than as soon as every week (72.8%), and so they reported the very best participation in social and mental actions. Although 61.2% reported no social actions, this proportion was markedly decrease than within the scientific teams, and so they displayed the very best proportions of engagement in a number of mental actions, notably on the stage of three actions (17.1%).
The dementia group was the oldest (M = 77.85, SD = 9.16) and had the bottom common years of training (M = 10.3, SD = 4.28). Women comprised 57.7% of this group. This group confirmed the bottom ranges of engagement throughout all exercise domains. Only 41.7% reported partaking in bodily exercise greater than as soon as every week, whereas 37.4% reported rarely or by no means being bodily lively. Social inactivity was particularly pronounced, with 84.8% reporting no social actions. Intellectual engagement was additionally decreased, with the very best proportion reporting no mental actions (39%) and the bottom proportion taking part in three actions (8.9%).
The Parkinson group had a imply age of 75.36 years (SD = 8.50) and a mean of 10.72 years of training (SD = 4.75). Women accounted for 49.4% of the group. Physical exercise ranges have been intermediate between the normative and dementia teams, with 51.4% partaking greater than as soon as every week and 30.5% reporting little or no exercise. Social participation was restricted, with 77.3% reporting no social actions. Intellectual engagement appeared considerably higher preserved in comparison with the dementia group, with comparatively balanced participation throughout one and two actions (27.4% and 29.6%, respectively), though participation in three actions remained modest (12.6%).
Finally, the stroke group had a imply age of 72.95 years (SD = 9.38) and a mean of 10.99 years of training (SD = 3.99). Women represented 47.9% of the group, the bottom proportion among the many 4 teams. Physical exercise was decreased in comparison with the normative group, with 51.1% partaking greater than as soon as every week and 28.2% reporting rarely or by no means being lively. Social inactivity was excessive (76.3%), although barely decrease than within the dementia and Parkinson teams. Intellectual exercise ranges have been comparatively just like the Parkinson group, with a average distribution throughout one (28.7%) and two actions (26.2%), however decrease engagement in three actions (13.1%) in comparison with the normative group. Descriptive statistics for the previous indicators and the cognitive scores of every group are offered in
Table 1 and
Table 2, respectively.
3.2. Structural Model and Measurement Invariance
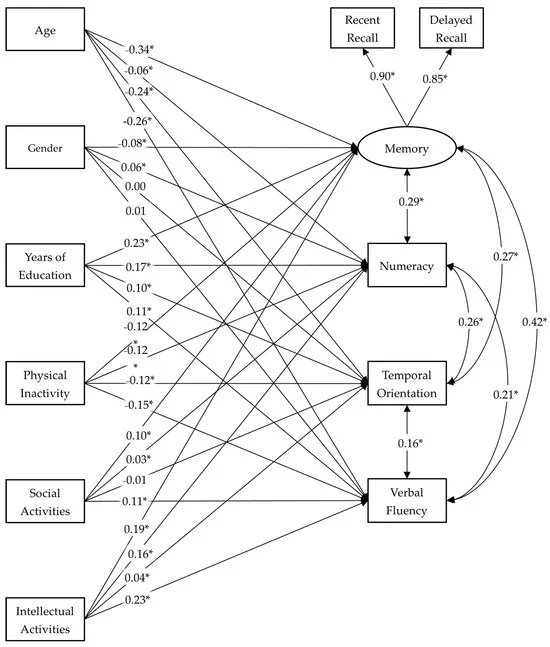
First, the MIMIC mannequin was estimated on the overall pattern. Fit indexes for the mannequin confirmed glorious match to the info: χ
2 (8) = 93.941,
p < 0.001, CFI = 0.997, RMSEA = 0.025, [90% CI 0.021–0.030] and SRMR = 0.004. Standardized parameters of the overall pattern mannequin are proven in
Figure 1, and correlation coefficients amongst exogenous variables are displayed in
Table 3.
After the mannequin was established and estimated on the overall pattern, the outcomes of estimating configural, metric and scalar invariance point out partial measurement invariance throughout analysis teams. Nevertheless, the estimated fashions demonstrated an sufficient match to the info. Fit indexes for the traditional invariance routine are displayed in
Table 4.
The moderating impact of the group on the relationships between the variables within the mannequin was studied by sequentially eradicating the parameter restrictions indicated within the modification indices. Therefore, the primary impact that was left free to estimate was the numeracy coefficient on mental actions. Subsequently, the coefficient of temporal orientation on bodily inactivity, the coefficient of temporal orientation on mental actions, the coefficient of numeracy on bodily inactivity, and, lastly, the coefficient of temporal orientation on age. This final mannequin was retained for subsequent evaluation of the differentiation of results throughout diagnostic teams, on condition that the match indices present a very good approximation to the match of the metric mannequin of the invariance routine. The match indices for the sequential elimination of parameter restrictions from the scalar mannequin are offered in
Table 5.
Regarding the free estimated coefficients, bodily inactivity was negatively related to arithmetic efficiency in all teams, though the magnitude of the affiliation diversified significantly. The impact was smaller within the normative group, whereas stronger unfavorable associations have been noticed within the scientific teams, particularly amongst individuals with dementia and stroke, adopted by individuals with Parkinson’s illness.
In distinction, mental actions confirmed a optimistic affiliation with arithmetic in all teams, with notably higher results in scientific populations. The strongest affiliation was noticed within the dementia group, whereas the Parkinson’s and stroke teams additionally confirmed stronger results than the normative group, suggesting that participation in intellectually stimulating actions could also be notably related for sustaining calculation means in individuals with neurological situations.
For temporal orientation, the sample was totally different. Physical inactivity was not considerably associated to orientation within the normative group however confirmed important unfavorable associations in all scientific teams, once more with the strongest impact within the dementia group.
The affiliation between mental actions and temporal orientation was comparatively decrease and extra diagnosis-specific. In the normative and Parkinson teams, the connection was not statistically important. By distinction, it was important within the dementia and stroke teams, though the magnitude remained modest. This sample means that mental actions are extra strongly related to temporal orientation in situations characterised by higher cognitive impairment.
Finally, age was negatively related to temporal orientation throughout all teams, with extremely important relations (all
p < 0.001). The magnitude of the affiliation was comparatively related within the normative, dementia, and Parkinson teams, indicating a constant age-related decline in orientation skills no matter analysis. The affiliation was considerably weaker within the stroke group. Overall, age seems to exert a strong and broadly comparable affect on temporal orientation throughout diagnostic classes, whereas lifestyle-related elements present extra pronounced variability of their influence. The freely standardized coefficients in every group are proven in
Table 6.
4. Discussion
In accordance with the theoretical framework of cognitive enrichment, a number of researchers have proposed the speculation that engagement in social and mental actions fosters the preservation of cognitive functioning throughout maturity and in late life [
70,
71,
72,
73].
This examine aimed to look at the associations of life-style, operationalized as bodily inactivity and participation in social and mental actions, on cognitive operate in the newest information from older adults within the SHARE undertaking, specifying the domains of reminiscence, arithmetic, temporal orientation, and verbal fluency. The specification of this mannequin comes from earlier analysis. The primary goal of this examine was to check the moderating results of the diagnostic group on the consequences of background elements inside this predictive mannequin of cognitive functioning, differentiating between sufferers with out a analysis, sufferers with dementia, sufferers with Parkinson’s illness, and sufferers who had suffered a stroke.
Results from this examine present that the predictive mannequin of cognitive functioning had a superb match within the normal pattern and achieved partial measurement invariance throughout diagnostic teams [
69], indicating that whereas the general cognitive construction was comparable, a number of structural relationships differed meaningfully between teams. Descriptive outcomes revealed clear demographic and life-style variations: the normative group was youthful, extra educated, and extra actively engaged in bodily, social, and mental actions, whereas the dementia group was the oldest and least lively throughout domains. Parkinson’s and stroke teams confirmed intermediate profiles, although each offered decreased exercise engagement in comparison with wholesome people.
Regarding the associations of predictors on cognitive measures, life-style elements exhibited differential results throughout diagnoses. Physical inactivity was negatively related to numeracy in all teams, however its influence was considerably stronger within the scientific group, notably in stroke and dementia, in comparison with the normative group. In this line, the earlier proof signifies the effectiveness of physical-activity interventions on stroke, Parkinson’s, and dementia [
74,
75,
76]. Similarly, mental actions have been positively related to numeracy throughout all teams, but the magnitude of this affiliation was markedly bigger amongst people with dementia, adopted by Parkinson’s and stroke sufferers. This means that mental engagement might play a extra pronounced compensatory or protecting position in scientific populations. In this line, cognitive coaching interventions additionally confirmed proof in sustaining cognitive efficiency in people with dementia, stroke, and Parkinson’s illness [
77,
78,
79].
For temporal orientation, the sample was extra diagnosis-specific. Physical inactivity confirmed no important affiliation within the normative group however demonstrated important unfavorable relations in all scientific teams, particularly amongst people with dementia. Intellectual actions have been unrelated to temporal orientation in wholesome and Parkinson teams, but confirmed modest however important optimistic associations in dementia and stroke teams. In distinction, age exerted a strong and constant unfavorable affiliation with temporal orientation throughout all teams, with solely barely weaker results within the stroke group.
Overall, the outcomes point out that though age-related cognitive decline follows a comparatively secure sample throughout diagnostic classes, the affect of modifiable life-style elements varies considerably relying on the underlying well being situation. Clinical teams seem extra delicate to each the unfavorable affiliation of bodily inactivity and the optimistic affiliation of mental engagement, supporting the notion that cognitive ageing will not be homogeneous however condition-specific. However, this examine additionally offered sure limitations. First, using cross-sectional information does probably not enable for the examine of causal relationships, because the precept of priority will not be fulfilled. It restricted the examine to attract exploratory conclusions in regards to the relationships between the variables, and it doesn’t assure the existence of a potential reverse impact or bidirectional relationship. Future analysis strains must be centered on the examine of the directionality of results by utilizing longitudinal information. Additionally, the predictor measures had some lacking information given the size of the interview and the big variety of variables to be evaluated, which is frequent in one of these information. On the opposite hand, cognitive functioning measures might current ceiling results on the wholesome group as they’re derived from the MMSE, which has been demonstrated to discriminate higher on scientific populations [
80]. Lifestyle indicators are based mostly solely on a depend of actions participated in through the previous yr, with out distinguishing between topics based mostly on frequency of participation. Lastly, the explicit variable employed to create analysis clusters may very well be extra particular to the response to dementia, because it contains each type of dementia analysis or senile situation in the identical group. Similarly, the group identified with stroke doesn’t take note of the variability that would exist relying on the severity of the case resulting from response time, extent, and affected areas. This might result in variations within the influence on particular domains [
57]. Additionally, a limitation of the structural mannequin (and by extension of most predictive fashions) is the analytical difficulties to deal with numerous probably confounding variables, comparable to illness severity and period; medicine results; socioeconomic standing; melancholy; cardiovascular threat; purposeful standing; and so forth and so forth. This should be acknowledged as a limitation of the present examine.