This web page was created programmatically, to learn the article in its unique location you may go to the hyperlink bellow:
https://wwwnc.cdc.gov/eid/article/32/2/25-1530
and if you wish to take away this text from our website please contact us
Disclaimer: Early launch articles will not be thought-about as remaining variations. Any modifications shall be mirrored within the on-line model within the month the article is formally launched.
Author affiliation: World Health Organization (WHO) Health Emergencies Programme, Geneva, Switzerland (H. Laurenson-Schafer, M. McMenamin, L.Okay. Ebbarnezh, R. Lewis, L. Subissi, A. Hosha, O. le Polain de Waroux); WHO Health Emergencies Programme, Regional Office for the European Region, Copenhagen, Denmark (I. Karagiannis, M.-A. Widdowson); WHO Health Emergencies Programme, Regional Office for the Western Pacific Region, Manila, Philippines (V. Biaukula); WHO Health Emergencies Programme, Regional Office for the South-East Asian Region, New Delhi, India (M. Kato); WHO Health Emergencies Programme, Regional Office for Africa, Brazzaville, Republic of the Congo (M. Muteba, F. Sanni); WHO Health Emergencies Programme, Regional Office for the Eastern Mediterranean Region, Cairo, Egypt (J.D. Naiene); WHO Health Emergencies Programme, Regional Office for the Americas, Washington, DC, USA (T. Dorji)
In September 2023, an outbreak of a brand new pressure of monkeypox virus (MPXV) emerged within the nonendemic Sud-Kivu province of the Democratic Republic of the Congo (DRC); the outbreak was pushed by sustained human-to-human transmission (1). Mpox circumstances beforehand reported within the DRC described outbreaks linked to zoonotic spillover in forested areas (2). The sustained human-to-human transmission within the 2023 outbreak led to proposed designation of a brand new MPXV subclade, clade Ib (1). Subsequent unfold to nations neighboring the DRC (3) prompted the World Health Organization (WHO) to declare a second public well being emergency of worldwide concern for mpox on August 14, 2024 (4). We collated knowledge from travel-related circumstances and their contacts reported to WHO to explain transmission dynamics, estimate secondary assault fee (SAR), and assist outline threat elements for clade Ib MPXV an infection.
By June 19, 2025, MPXV clade Ib had been reported from 14 nations in Africa. Travel-related circumstances, as outlined by WHO (5), have been reported from 19 nations outdoors of Africa and led to secondary circumstances in 8 of the vacation spot nations.
Figure 1

Figure 1. Transmission dynamics amongst world travel-related mpox circumstances brought on by clade Ib monkeypox virus. Yellow dots characterize nation of publicity; arrows characterize course of journey for mpox circumstances reported as of…
We used case knowledge that was shared with WHO below the provisions of the International Health Regulations (2005) (6) or revealed individually. We collated knowledge from 127 mpox circumstances, 124 confirmed and three suspected; 89 have been travel-related, 34 have been secondary, and 4 have been unlinked. Of the 89 travel-related circumstances, 70 case-patients reported having been uncovered in Africa and 18 outdoors Africa; 1 had unknown publicity origin (Figure 1). All imported circumstances have been amongst adults, besides 1 of unknown age (lacking knowledge); 88 circumstances had intercourse knowledge accessible, 67 (76%) have been males and 21 (24%) have been girls; 25 travel-related circumstances led to 34 secondary circumstances within the nation of notification, together with circumstances amongst 6 males, 19 girls, and 6 youngsters (<17 years of age). Among secondary circumstances, 15/25 (60%) adults reported sexual contact or probably sexual contact with the index case (i.e., unspecified contact with the index case’s companion).
Figure 2
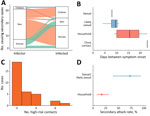
Figure 2. Characteristics and transmission dynamics amongst world travel-related mpox circumstances brought on by clade Ib monkeypox virus. A) Sankey diagram of secondary transmission occasions amongst 33 transmission occasions and secondarily contaminated individuals….
Of the 33 secondary circumstances with knowledge accessible for each index and secondary circumstances, most (73%) resulted from males, who transmitted MPXV to principally girls and kids, adopted by girls (21%), who contaminated principally males and kids. Secondarily contaminated youngsters (6%) contaminated 1 youngster and 1 man (Figure 2, panel A). Using 14 case pairs, we estimated that the imply serial interval (SI) for an infection was 12 (95% CI 4–27) days. We estimated that the SI for sexual and sure sexual contact was 9 (95% CI 5–14) days, which was shorter than the SI for nonsexual family contact, 15 (95% CI 8–29) days (Figure 2, panel B). That SI distinction may partly be due to the shorter incubation interval and better infectious dose for sexual transmission (7; F.Okay. Kaiser et al., unpub. knowledge., https://doi.org/10.1101/2025.08.14.669880).
Contact knowledge have been accessible from 50 circumstances, and we have been capable of disaggregate threat standing of contacts for 32 of these circumstances. We outlined high-risk contacts as family members, sexual contacts, or each. When no additional data was accessible, reporting nations outlined high-risk contacts. Using these knowledge, we recognized a complete of 74 high-risk contacts from 33 circumstances, 1 of which didn’t have sufficient data accessible to disaggregate additional into contact sort (Figure 2, panel C). Of the 25 major circumstances from whom secondary transmission was reported, a median of 1 (vary 1–4) secondary case occurred. We estimated the SAR for family contacts was 17% (95% CI 8%–31%) and for sexual contacts was 73% (95% CI 39%–94%) (Figure 2, panel D). No secondary circumstances have been reported amongst group contacts or contacts in healthcare settings.
The first limitation of our evaluation is the small pattern measurement as a result of data was lacking for some circumstances. Second, the sexual contact SAR is primarily restricted to transmission between spouses or companions, and the excessive estimate would possibly mirror repeated sexual publicity, extended shut contact throughout the family, or each, along with a attainable underreporting of sexual contacts outdoors the family. Finally, travel-associated circumstances could possibly be missed, particularly in nations the place mpox is strongly stigmatized, and our estimates won’t be generalizable past the settings described.
Our outcomes spotlight that shut contact is a key driver of MPXV clade Ib outbreaks and present that sexual contact carried the best transmission threat, adopted by family contact. We discovered no proof of an infection threat past settings the place contact was probably shut and extended. Other research have additionally acknowledged the function of sexual contact as essentially the most environment friendly MPXV transmission route (8,9). Of be aware, secondary family circumstances have been recognized in the course of the MPXV clade Ib outbreak reported right here, however in the course of the 2022–23 clade IIb outbreak, such occasions have been uncommon; earlier than August 2024, WHO recorded solely 15 (0.2%) of seven,794 mpox circumstances in youngsters <15 years of age amongst these uncovered within the family (knowledge not proven). Whether that disparity displays variations in family and social contact buildings or intrinsic viral properties stays unclear. The greater threat related to sexual publicity and family contact ought to inform response methods and precedence interventions for populations most in danger.
Dr. Laurenson-Schafer is a knowledge analyst for well being emergencies working at WHO, Geneva, Switzerland. His analysis pursuits concentrate on the usage of knowledge science within the context of illness surveillance, outbreak and emergency response, and humanitarian settings. Dr. McMenamin is a knowledge scientist within the WHO Health Emergencies Programme in Geneva. Her analysis pursuits concentrate on outbreak analytics and surveillance in emergency response.
WHO Mpox Collaborative Surveillance Group: Steve Kerr (CPC Analytics, Berlin); Yurie Izawa (WHO Health Emergencies Programme, Headquarters, Geneva, Switzerland); Esther Muwanguzi, Sara Hollis, Penelope Gorton (WHO Health Emergencies Programme, Regional Office for Africa, Brazzaville, the Republic of Congo); Mahmoud Hassan, Shaza Mohammed, Sherein Elnossery, Basant Mohamed (WHO Health Emergencies Programme, Regional Office for the Eastern Mediterranean Region, Cairo, Egypt); Jeffrey Pires, Kareena Hundal, Nhu Nguyen Tran Minh (WHO Health Emergencies Programme, Regional Office for the European Region, Copenhagen, Denmark); Rajkrishna Ravikumar, Christian Hertlein, Silvano Barbosa De Oliveira (WHO Health Emergencies Programme, Regional Office for the Americas, Washington DC, United States of America); Stefany Ildefonso Acuna, Pavana Murthy, Pushpa Ranjan Wijesinghe, Manish Kakkar (WHO Health Emergencies Programme, Regional Office the South-East Asian Region, New Delhi, India); Tika Ram, Sean Casey, and Chen Zhongdan (WHO Health Emergencies Programme, Regional Office for the Western Pacific Region, Manila, Philippines).
Top
This web page was created programmatically, to learn the article in its unique location you may go to the hyperlink bellow:
https://wwwnc.cdc.gov/eid/article/32/2/25-1530
and if you wish to take away this text from our website please contact us